
What is Asthma?
Asthma is a condition that affects the small air passages in the lungs. In asthmatics, the airways become over-sensitive and react to things that would not normally cause a problem, such as cold air or dust.
Wheezing is very common in babies and toddlers yet not all children with wheeze go on to develop asthma. Many children's symptoms resolve with age but even in these cases a lifelong predisposition to lower airway irritability is thought to persist.
Asthma affects each person differently and can sometimes be unpredictable. Asthma attacks are more likely to occur in those with moderate-severe asthma but asthma attacks can also occur in people with mild asthma.
Pathophysiology of Asthma
Muscles around the wall of the airways tighten up, making them constrict and reducing the airflow in and out of the lungs. The lining of the airways becomes swollen (just like your nose during a cold) and sticky mucus is produced which further clogs up the breathing passages. With the airways narrowed like this, you can see why it becomes difficult for air to move in and out and why the chest has to work so much.
Tightening of muscle around the airways can happen very quickly and is the most common culprit in mild asthma. Fortunately this can be reversed quickly too by using a reliever inhaler. However, the airway swelling and accumulation of mucus described above occur much more slowly and usually require daily preventer inhalers or tablets. These symptoms take longer to control and are a particular problem in serious episodes of asthma.
Epidemiology of Asthma
Asthma is a huge burden globally accounting for approximately 340 million individuals worldwide. It has a prevalence of 7% in Irish adults and 21% in Irish children which amounts to about 460,000 people in Ireland.
Based on the HSE figures from 2011, about 248,000 people in Ireland have non-controlled asthma. This grouping experience more frequent asthma exacerbations, are more likely to require emergency care for their asthma and are at higher risk of negative outcomes. Every year in Ireland, there are approximately 50,000 asthma attendances in GP out of hours services and 20,000 asthma attendances to Irish hospital emergency departments. 5,000 of these patient require admission to hospital while 100 are admitted to ICU. There are roughly 50 deaths per year from asthma in Ireland which translates to one death every week. Most of these deaths occur in the community.
Difficult to Treat Asthma
This refers to those with a confirmed diagnosis of asthma that have persistent, uncontrolled asthma symptoms and exacerbations despite high dose preventative medication. Despite about 17% of patients fitting the criteria for difficult-to-treat asthma it is estimated that only 3.6% of asthmatics actually have severe asthma. This disparity likely reflects poor asthma control as a result of confounding factors such a poor medication adherence, inadequate inhaler technique, smoking history or suboptimal management of comorbidities such as obesity and rhinitis.
Airborne Allergies and Asthma
Does treating Allergic Rhinitis improve Asthma control?
Chronic asthmatics commonly suffer from allergies to airborne allergens such as House Dust Mite, Pollen, Animal Dander and mould spores. In fact, up to 90% of asthmatics have allergic rhinitis and up to 40% of those with allergic rhinitis have asthma. This causes inflammation and mucosal swelling within the upper airways of the nose and sinuses which can be detrimental to the control of asthmatic symptoms.
The treatment of nasal inflammation in asthmatics has been shown to improve outcomes. This highlights the importance of assessing for both asthma and rhinitis in these patients for asthmatics with allergic rhinitis. A ‘united airways disease' approach to management is the more favoured approach in recent years. Management should include avoidance measures of the particular allergic trigger and treatment of their nasal symptoms and underlying allergy.
The impact of Hay Fever on Asthma
Asthma sufferers with pollen sensitivity may have noticed that their asthmatic symptoms can substantially worsen during hay fever season. This is not surprising as pollen that enters the sensitive and reactive airways of asthmatics will irritate and precipitate an allergic response in the lungs just as it does in the nose, eyes and skin. If the pollen levels are sufficiently high an asthma attack can be triggered in susceptible individuals.
In addition to pollen directly interacting with the lower airways of the lungs, there is strong clinical evidence that poorly controlled allergic rhinitis worsens asthmatic symptoms. Propagation of inflammation from the upper airways to the lower airways occurs both via postnasal secretions and the systemic circulation.
This makes it particularly important to manage hay fever and rhinitis symptoms in those who also have asthma. This results in better outcomes for both conditions. Additional options for hay fever treatment are now available such as desensitisation immunotherapy to pollen and Rhinolight UV endonasal phototherapy.
The impact of House Dust Mite allergy on Asthma
Asthmatic patients and the parents of asthmatic children often comment that their symptoms worsen in 'dusty environments' such as the houses of some friends or family and dusty settings such as building sites. The dust found in the air at a building site consists of irritant particles so it is not surprising that the sensitive and reactive airways of asthmatics are triggered in these settings. However, house dust mite allergen found in high quantities in household environments will also act as a potent trigger in asthmatics with house dust mite allergy.
Dust mite allergen directly interacts with the lower airways to trigger asthmatic symptoms. It also causes inflammation and swelling of the upper airways of the nose and sinuses which also contributes to the exacerbation of asthmatic symptoms. Propagation of inflammation from the upper airways to the lower airways occurs both via postnasal secretions and the systemic circulation. The immunological mechanism is illustrated in the graph below.
In these cases it is very important to minimise house dust mite exposure and to control upper airway symptoms in order to optimise asthma control. In patients with significant asthma associated with a coexisting house dust mite allergy, desensitisation immunotherapy to house dust mite can often be used to eliminate this allergy and improve asthma control.
What causes Asthma?
- It can start at any time of life, although it most often begins in childhood.
- Sometimes it runs in families along with other atopic conditions in the family.
- Some children's asthma is related to other conditions, such as eczema, hay fever and allergies.
- Adult-onset asthma may develop after a respiratory tract infection.
- Many aspects of modern lifestyles such as changes in housing, diet and a more sterile home environment may have contributed to the rise in asthma over the last few decades.
What are the Symptoms of Asthma?
- Difficulty breathing/shortness of breath.
- A tight feeling in the chest.
- Wheezing.
- Coughing - a cough alone does not mean asthma.
- particularly at night or early hours of the morning
- during cold weather
- during exercise
Signs of Poorly Controlled Asthma
- Daily symptoms such as cough, wheeze and shortness of breath.
- Frequent reliance on reliever inhalers such as Ventolin.
- Repeated courses of oral steroids.
- Frequent hospital admissions.
Treatment of Chronic Asthma Symptoms
It is important to ensure that asthma is diagnosed and treated appropriately based on its severity. Not only is poorly controlled asthma very disruptive to a persons life but it can also be life threatening at any age. Children with asthma should have an Asthma Action Plan in order to help guide management to reduce the number of asthma flare ups and ensure the right treatment in the event of asthma episodes (sometimes called asthma attacks).
In cases where an allergic trigger (house dust mite, pollen, mould, feather or animal dander) is suspected it is important to carry out skin prick allergy testing or IgE specific blood tests.
Reliever asthma medications
Salbutamol (Ventolin) inhalers are the most commonly used 'reliever' medication in Asthma. They are known as 'short acting beta agonists' as they work by binding to beta 2 adrenergic receptors in the lungs to helps open up the airways. They are fast acting and usually provide relief for several hours.
Preventer asthma medications
Inhaled corticosteroid inhalers (Becotide, Flixotide, Ciclesonide etc) are the most commonly used 'preventer' medication option for asthma symptoms. In order to be effective they must be used on a daily basis. We recommend the use of a spacer (available over the counter) for all ages while taking these medications as it reduces side effects such as oral thrush and greatly improves the efficacy of the medication.
Leukotriene receptor antagonists such as montelukast (Singulair) are sometimes used as either an alternative to inhaled corticosteroid inhalers in mild asthma or as an adjunct in more significant asthma.
Immunotherapy for Asthma
The most recent international guidelines recommend immunotherapy be considered for mild-moderate asthmatics sensitised to dust mite. In this cohort of asthma patients immunotherapy may significantly reduce symptoms and medication requirements. It is typically most effective in patients under the age of thirty and it is usually very well tolerated.
Treatment of an Acute Severe Asthma Attack
Under 12's
- Sit the child upright.
- Give up to 6 puffs of Salbutamol (Ventolin) via a Spacer over 6 minutes.
- Call for medical help immediately.
- If there is no improvement then dosing can repeated every 20 minutes.
Over 12's
- Sit the person upright.
- Give up to 10 puffs of Salbutamol (Ventolin) via a Spacer over 10 minutes.
- Call for medical help immediately.
- If there is no improvement then dosing can repeated every 20 minutes.
Asthma Prognosis
With the right treatment, nearly all children with asthma will be able to participate in sport and lead active lives. Many children improve with age and almost half seem to 'grow out' of their asthma. Despite this a predisposition towards sensitive airways and asthmatic symptoms usually persists. About half of those who have recovered from asthma will relapse in their 30's or 40's.
Asthma Information for Health Professionals
Asthma Treatment Guidelines for Health Professionals
A stepwise treatment is recommended for asthma as shown below in the GINA guideline illustration. All patients should be given a salbutamol SABA reliever for rapid symptomatic relief.
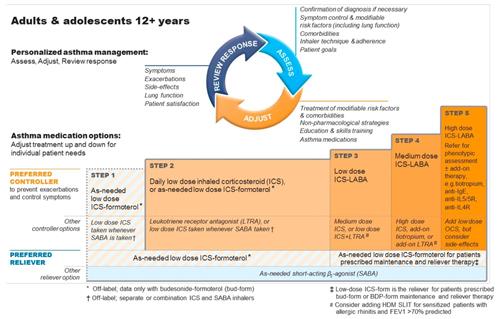
Controller Medication
Step 1: A combination ICS-formoterol inhaler (eg Symbicort) taken as required is now first line.
Step 2: If symptoms persist continue ICS-LABA PRN or increase to daily low dose ICS. Alternatively use LTRA.
Step 3: Increase to daily low dose ICS-LABA. Alternatively use medium dose ICS alone or low dose ICS + LTRA.
Step 4: Increase to medium dose ICS-LABA. Alternatively use high dose ICS +/- LABA +/- LTRA
Step 5: High dose ICS-LABA +/- LAMA +/- LTRA +/- anti-IgE, Anti-Il5R, Anti-Il4R. Refer for Asthmatic Phenotyping.
Immunotherapy
The most recent GINA (Global Initiative for Asthma) guidelines recommends immunotherapy be considered for asthmatics sensitised to dust mite. Immunotherapy has been shown to significantly reduce symptoms and medication requirements and is also recommended by the ARIA (Allergic Rhinitis and its impact on Asthma) guidelines for these patients. However, it should not be started in patients with severe asthma due to the risk of precipitating a severe asthma exacerbation.
Immunotherapy involves exposing a patient to minute quantities of the allergen trigger allowing the immune system to build up a tolerance. It is highly effective in patients under thirty years of age and very well tolerated. It can be given as a subcutaneous injection or as a sublingual tablet. Sublingual therapy is used predominantly in Ireland and is currently available for grass pollen, dust mite and tree pollen. Compliance is crucial and regular follow up advised. It is usually a three year process whereby the patient takes it daily.
Further Treatment Options in Severe Asthma
In this cohort of patients it is imperative to consider targeted therapies. To be a candidate for biologic therapy their phenotype needs to be Type 2 inflammatory Severe Asthma. MDT involvement here improves recognition of phenotypes allowing the most suitable biologic therapy choice.
Monoclonal Antibodies (MABs) inhibit a target molecule in the inflammatory process such as IgE, IL-5 (anti-eosinophil), IL-5R, IL-4R and IL 13. This is only effective if that specific inflammatory pathway is underlying the patient’s asthma. Unfortunately, there are currently no biologic options for non-type 2 inflammatory asthma.
Assessment of Difficult to treat Asthma
When assessing difficult-to-treat asthma it is important to revisit the diagnosis. It is imperative to consider if there are any features suggestive of a differential or coexisting diagnosis. To assess symptom control, patient questionnaires can be utilised such as the Asthma Control Questionnaire.
Spirometry
Spirometry would be used to confirm the diagnosis of asthma. This will establish lung function likely showing a reduced FEV1/FVC ratio indicating expiratory airflow limitation. Variability in lung function increases in poorly controlled asthma and so it is likely that >12% and >200ml reversibility in FEV1 would further confirm the diagnosis. A bronchial provocation test can be considered to assess airway hyperresponsiveness.
Allergy Testing
Skin prick testing and/or serum specific IgE testing should be carried out to identify allergies to common airborne allergens such as house dust mite, pollen and mould spores.
Asthmatic Phenotyping for Severe Asthmatics
The GINA guidelines recommend referral for Phenotyping in the management of severe asthmatics. Phenotyping is a way to characterise both the clinical and functional features of a patient’s asthma along with the distinct molecular pathway involved referred to as the endotype.
Once a diagnosis of severe asthma is substantiated, the next step in the assessment process is to establish the inflammatory phenotype and to ascertain the patient’s suitability for targeted biologic treatment. The intention is to prepare an effective personalised therapeutic approach. Two main phenotypes have been established based on the presence or absence of Type 2 inflammation.
- Type 2 inflammation in asthma is distinguishable due to the predominance of IL-4, IL-5 and IL-13 which stimulate the production of Eosinophils and often atopy (elevated IgE). Moreover, Type 2 inflammation is often accompanied by a raised Fractional Exhaled Nitric Oxide (FeNO). Serum Periostin can be an additional biomarker for Type 2 inflammation.
- Non-type 2 asthma is often characterised by neutrophilia but can be paucigranulocytic with no clear elevation in inflammatory cells. Despite obesity playing a considerable role in the development and control of severe asthma, there is also a distinct non-type 2 inflammatory obesity-related phenotype.
A proportion of asthmatics have type 2 inflammation underlying their asthma and fall into the mild-moderate asthma cohorts and generally show an excellent response to ICS. Approximately 50% of the severe asthma subset show evidence of type 2 inflammation but despite this they are often refractory to ICS treatment thus requiring maintenance oral corticosteroids.